
Two weeks before the DSM- 5 came out, the head of the National Institute of Mental Health (NIMH) said they weren’t going to use it.Insel They are replacing it, for the purposes of NIMH research, with their own system based on what we have learned about the brain in the last several decades: their Research Domain Criteria, RDoC.
In describing the RDoC system, one of its developers described the DSM as a system of “invented categories.” I too think its time to move beyond the DSM (as I have been practicing for over a decade). Now we have the NIMH saying likewise.
DSM-5 Reliability
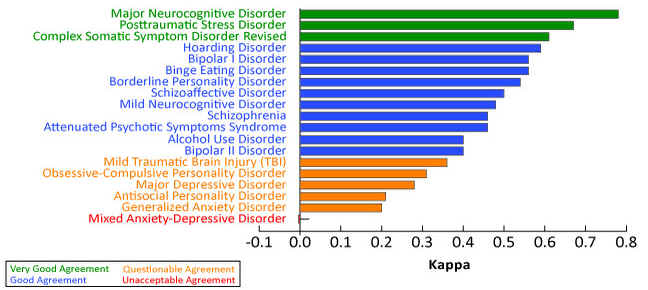
Research preceding the DSM-5 suggested that some psychiatric diagnoses don’t do their job very well. Different psychiatrists, using the same criteria, seeing the same patient, don’t arrive at the same diagnosis. The slide below is from a review of this issue in 2013.Stetka
In this graph, the green range reflects “very good agreement” between diagnosticians. The orange range diagnoses reflected “questionable agreement” between diagnosticians. Notice that this includes major depressive disorder and generalized anxiety disorder. (The “Mixed Anxiety-Depressive Disorder” was a new category being considered for DSM-5, but it was dropped because of the unacceptably low inter-rater agreement shown here).
Notice also that the diagnosis of Bipolar II is just slightly better than “questionable”.
Enter the NIMH’s RDoC
In describing their Research Domain Criteria (RDoC), the NIMH’s Bruce Cuthbert, Ph.D. quotes a prominent schizophrenia researcher who says “there is no such thing as schizophrenia. It is a syndrome. It is a collection of things that psychiatrists have grouped together.” (Here is a video of a 30 minute presentation by Dr. Cuthbert in which this quotation and those below appear).
Instead, he says that the NIMH is trying to “move forward . . . rather than making these symptom categories… that were defined in the absence of any knowledge about the brain, anywhere from 100 to 2000 years ago.” “Rather than inventing these other categories like schizophrenia or bipolar disorder and expecting the brain can match up with our cultural descriptions of what appears to be wrong.”
According to the NIMH website describing it, the RDoC is conceived as a dimensional system . . . spanning the range from normal to abnormal.” RDoC There are no specific cutoff points, although it is acknowledged that for clinical purposes there will have to be some point beyond which one thinks clinically, e.g. about went on to contemplate offering treatment. Likewise there are no cutoffs between domains. It is acknowledged that any given individual could have a complex blend of features across different domains.
Each domain reflects an aspect of human experience, and each includes within it several “constructs” which are recognized as artificial (human-imposed, not necessarily brain-based), as follows
| Human experience | RDoC Domain | Constructs within this Domain |
| Negative | Negative “valence” | fear, anxiety, loss, frustration |
| Positive | Positive “valence” | reward, motivation, habit |
| Thinking | Cognition | attention, perception, cognitive control, memory |
| Social interaction | Social processes | attachment, communication, perception of self and others |
| Sleep | Arousal/regulatory | circadian rhythm, sleep and wakefulness |
Each domain can vary from “normal” to “abnormal”. There are no official cut-offs to make “diagnoses” in this system.
Each domain can be approached on multiple levels of analysis:
- genes
- molecules
- cells
- circuits
- physiology
- behavior
- self-report
- experimental paradigms
Each construct above can be approached on each of these levels. Here’s the anxiety construct, for example (from the matrix on the RDoC page).
| Construct | Genes | Molecules | Cells | Circuits | Physiology | Behavior | Self-report | Paradigm |
| Anxiety | corticotropin releasing factor (CRF) | CRF, cortisol | Pituitary cells | BNST | Average cortisol and ACTH levels; potentiated startle | Avoidance | Beck Anxiety Inventory | Contextual threat, darkness, |
My Opinion
The concept of a mood spectrum ranging from “unipolar” to “bipolar” has been central to my way of thinking for over a decade, as reflected all over this website. That was not an admissible way of thinking in the DSM system. The DSM was based entirely on a system of categories which did not allow the idea of a continuum.
Although the RDoC is not a diagnostic system, it demonstrates that some of the best brain scientists in the United States have decided, collectively, to move away from the DSM because it is regarded as, frankly, ancient. The DSM does not correlate very well with research findings from genetics, brain anatomy, and brain function .The NIMH is basically announcing that we need to start all over again.
In the process of starting over, the NIMH has begun with a system that is expressly “dimensional”, which is the jargon term for “spectrum”. The NIMH has entirely abandoned the idea of discrete categories of illness that can be separated from one another with diagnostic criteria. Instead, as I see it, the RDoC system demonstrates that the NIMH team regards human experience and brain research findings as “spectra”, shading continuously from normal to abnormal, and shading continuously from one “construct” to another.
(updated 10/2013)